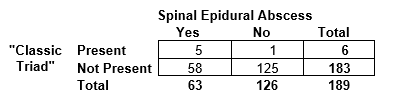
Spinal epidural abscess (SEA) is a rare but potentially devastating infection in the space next to the spinal cord. Davis et al(Davis, Wold et al. 2004) studied the accuracy of the “classic triad” of fever, spine pain, and neurologic deficit to diagnose spinal epidural abscess in emergency department patients. From the abstract: “Inpatients with a discharge diagnosis of SEA and a related ED visit before the admission were identified over a 10-year time period. In addition, a pool of ED patients presenting with a chief complaint of spine pain was generated; controls were hand-matched 2:1 to each SEA patient based on age and gender.” The results were as follows:
a. What is the sensitivity of the “classic triad” for spinal epidural abscess?
b. What is the specificity of the “classic triad” for spinal epidural abscess?
c. The authors’ Table 1 reports a positive predictive value of the “classic triad” as 5/6 or 83.3%. Do you agree with their calculation? Explain.
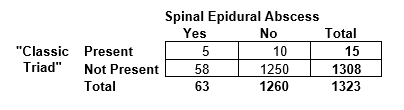
d. The authors do not provide the number of subjects in the “pool of ED patients presenting with a chief complaint of spine pain,” from which the control group was selected. Let’s suppose that the pool included 1260 patients with the same age and gender distribution as the cases and controls they selected and that within this group their control selection process was random. How would you use this information to obtain an alternative estimate of the positive predictive value?
a. Answer: 5/63 = 7.9%
b. Answer: 125/126 = 99.2%
c. Answer: We disagree. The positive predictive value is dependent on the pre-test odds, and in this case the pre-test odds were artificially set by the investigators at 1:2. Some students have argued that the calculation of positive predictive value is correct because in this study the prevalence of SEA was in fact 33%. But we think it is inappropriate to call the proportion with SEA in this study a prevalence. If you disagree, would you be OK with investigators doing a study that included zero controls and reporting a positive predictive value of 100%?
d. Answer: Knowing the size of the pool of spine pain patients can help us get a better estimate of the pre-test probability of SEA. In this case, we would simply multiply the No Spinal Epidural Abscess column by 10 to get a 2 × 2 table that more closely approximates what we might obtain with cross-sectional rather than case-control sampling. This would give a revised positive predictive value estimate of 5/15 = 33%. This would be a much better estimate of positive predictive value, but still only approximate, because the study design did not require that the SEA patients have a chief complaint of spine pain, as was required for the controls.
Back to all Chapter 2 Problems
Back to all Chapters
References
Davis, D. P., R. M. Wold, R. J. Patel, A. J. Tran, R. N. Tokhi, T. C. Chan and G. M. Vilke (2004). “The clinical presentation and impact of diagnostic delays on emergency department patients with spinal epidural abscess.” J Emerg Med 26(3): 285-291.